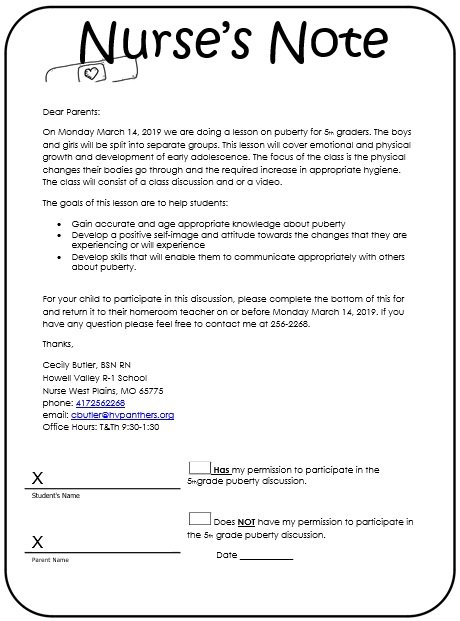
A nursing note template is used by nurses to take notes on every interaction they have with patients. In medical emergencies, the nurse is one of the front liners. Nurse notes are very important for the nurses because they administer drugs to patients in the hospital.
What is a nursing note?
Nursing note is formal documentation used to inform the medical professionals about the patient’s health. Nurses must make notes regarding their patients because they are the ones who spend the majority of the time with patients. They take notes on the basis of scribbles and notations.
Nursing note is considered as a shorthand technique of specifying any abnormalities or exceptions that are experienced by the patient. In order to make sure an effective communication between nurses and other healthcare staff, you should make nursing notes accurate and comprehensive.
Different types of nursing notes:
Let us discuss below the main types of nursing notes;
Ongoing documentation notes
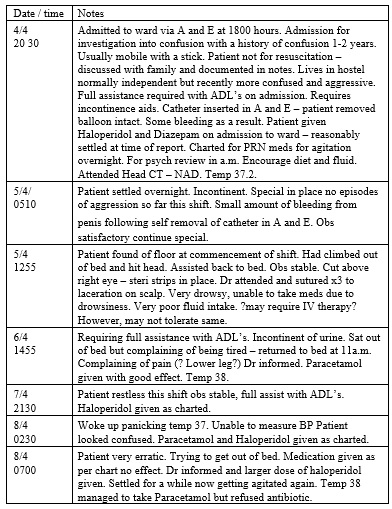
An ongoing documentation note is a routine documentation that states how nurse is taking care a patient regularly. With the help of these notes, throughout the entire course of the nurse medical therapy, they can keep check on the treatment and progress of patients.
Health notes
A health note is an essential note used to document the changes in patient, improvements, regressions, and any other side effects that patient may face due to treatment. These notes also include discharge notes, admission notes, and fall notes.
Incident notes
As its name implies, they are used in case of incidents and are considered complicated as they contain complex details. While writing these notes, focus on the events or happenings as it unfolds. They should well-written and well-engaged.
Behavior notes
These type of nursing notes are relevant to incident notes and considered as psycho-social. Nurses use them to keep track of patient’s behavior such as aggressive behavior, fights, and threats to others.
Communication notes
With the help of these nursing notes, hospital staff know more about the patient. Revealing some important information which is not readily known by other staff in the main purpose of communication note.
Death note
Death note is primarily direct nursing note. In case of accidental death, this note would be comprehensive.
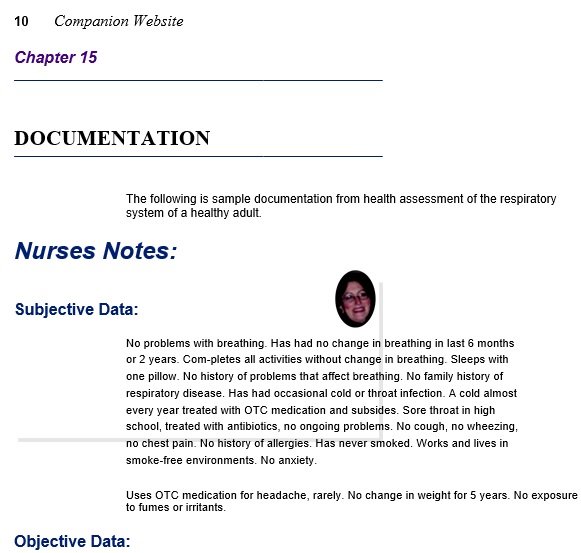
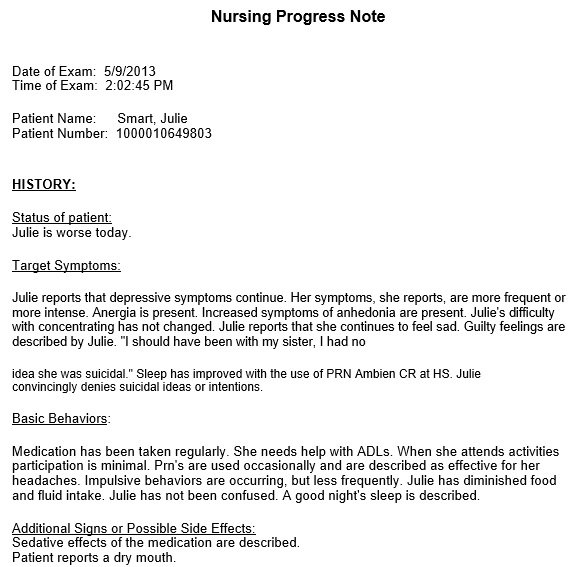
Progress notes on nursing:
Commonly speaking, nurses are patient advocates. They spend the most time with patients. Making nursing notes gives you a complete picture of the patient’s health. Then, other medical specialists and professionals can use this in making diagnoses or suggesting treatments. Moreover, while charting patients, these notes are a form of official documentation made by nurses. In your nurses’ notes templates, you write down essential information depending on the scribbling and notations you collect during your visits with the patients.
It is extremely important to keep accurate and thorough notes. It also maintains effective communication between you and the rest of the medical staff.

The benefits of writing nursing notes:
Nursing notes usually contain a patient’s general and basic information. It can include the following;
- The appearance of the patient
- Medical history of the patient
- Patient’s current medical condition
It also has information about a certain person involving your observations and your opinions depending on those observations. For example, after conducting nursing assessments and tests, many nurses make nursing progress notes.
Generally, these notes give details related to a patient’s overall medical status. These notes also assist you in keeping a record of your observations about patients. Along with your work, you should also include the behaviors and activities of your patient in your notes.
The details given by your notes assist you in monitoring any changes in a patient’s behavior and condition over a particular period of time. This way, you can determine what causes these changes.
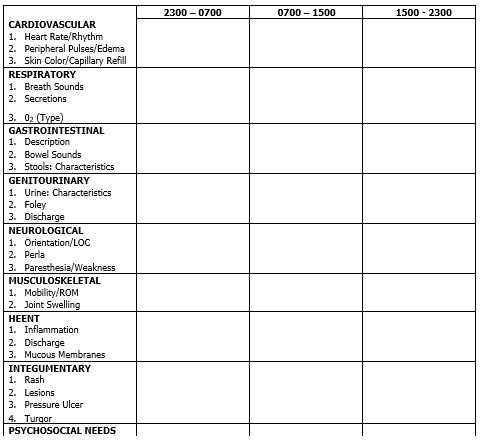
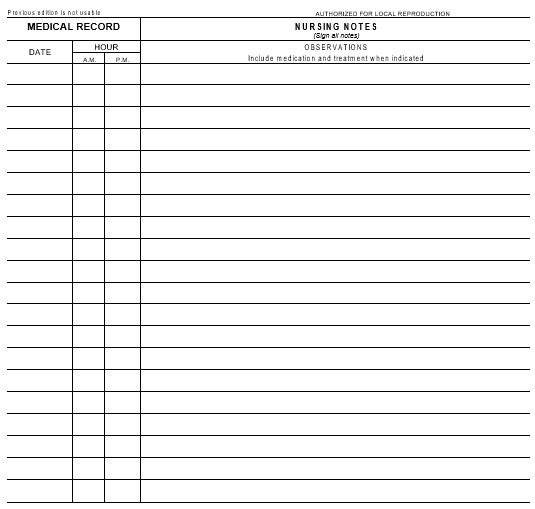
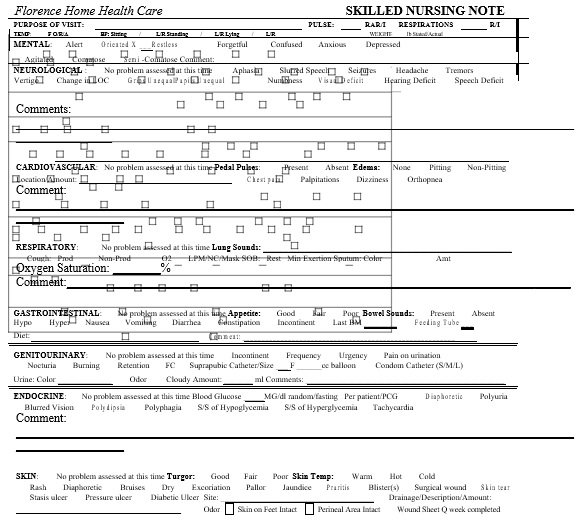
What to include in a nursing note?
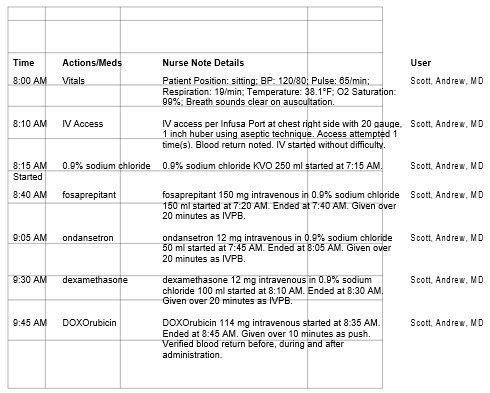
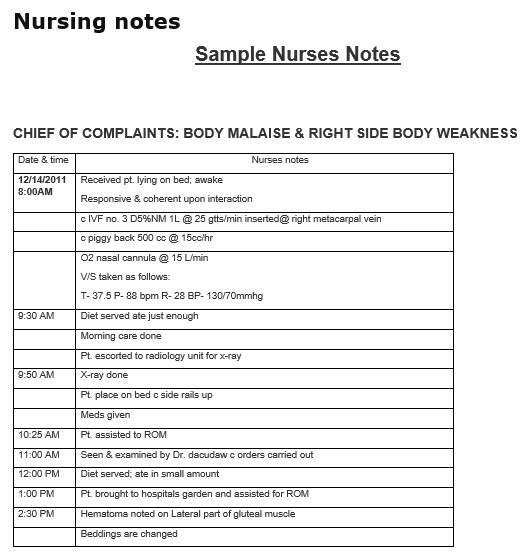
Nursing notes have pages along with the lines. They have title like “Progress Notes” or “Nursing Notes.” However, this document includes the following;
- The time and date
- The name of the patient
- Name of the attending nurse
- The reason for the patient’s visit
- The vital signs of the patient
- Your initial assessment of the patient
- Any diagnostics or labs requested
- An assessment of any medical interventions conducted
- Any significant instructions provided
- The family interactions that the patient has in the past
- Observations and recommendations
- Anything unusual that you have noticed
What not to include in a nursing note?
Never include personal sentiments in nursing notes just state factual information. However, you can verbally inform the medical professionals about the patient’s health. Here are some details that you shouldn’t include in the nursing note;
- Never include the patient’s personal details such as the information regarding their family members and friends.
- There is no need to state the dialogues about patients between the providers.
- Never include anything from the ISMP Abbreviation lists because this list can be misinterpreted. Some medication errors may also arise due to this list.
- It wouldn’t be good to state negativity about the staff. If there is any issues regarding the staffs then you should report it in such a way that won’t make any issue in the hospital.
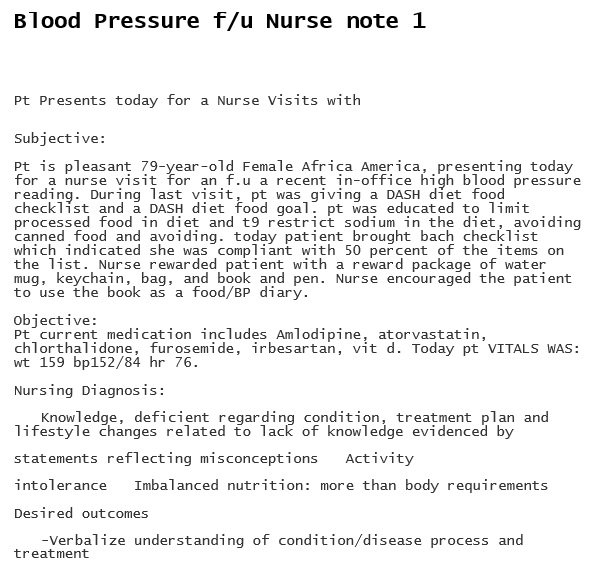
The most important information that you must include:
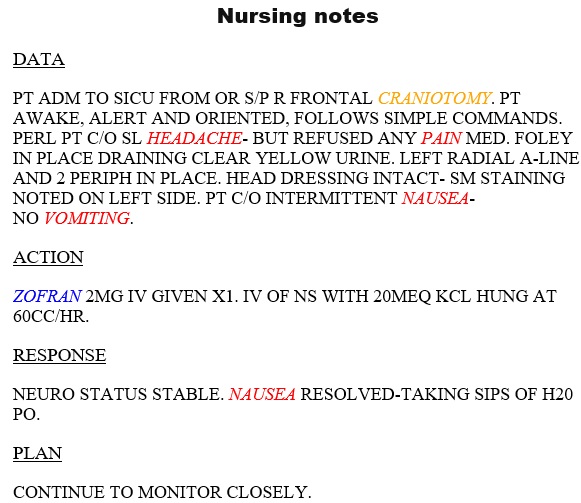
There are three main issues that you must mention each time you write these notes;
Description
In the description, explain what’s going on with your patient. Explain the patient’s condition in detail. Specify what you see, hear, smell, and felt as well as the remarks of the doctor.
Action
The actions that you or the doctor has taken in response to the patient’s condition explain them. This usually involves giving the medication, making sure the patient’s safety, and the like.
Response
Here, provide an explanation of how the patient responded to the actions taken. In this way, you identifies either the patient improves because of your actions or your actions have no effect.
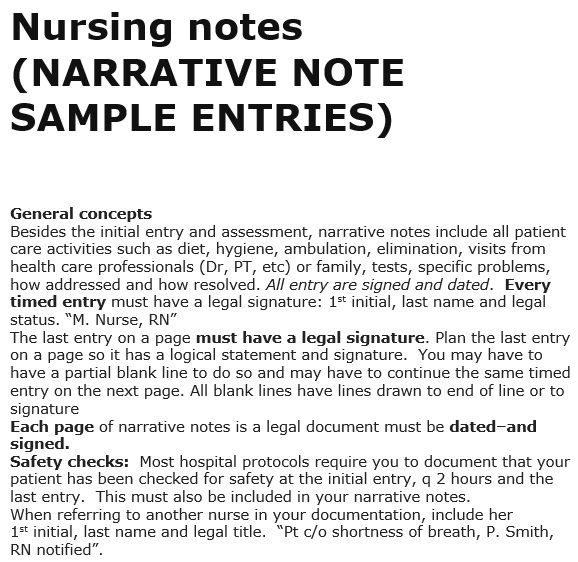
How to write a nursing note?
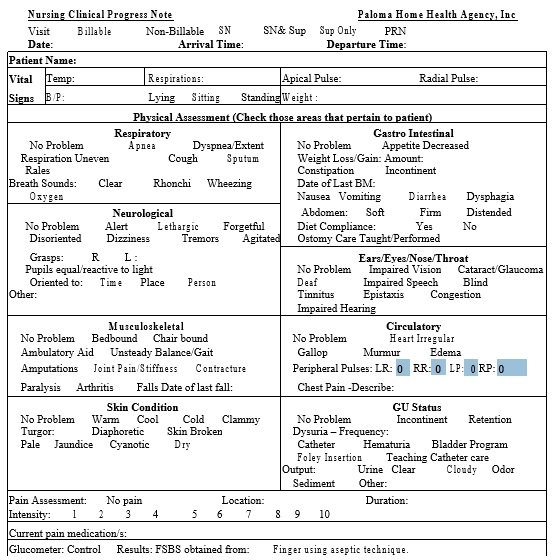
Nurse notes templates commonly include the following;
- Exact nursing evaluations or documentation
- In the condition of a patient, observed changes
- Care or treatment provided to the patient
- To support the clinical team, other related information
Consider the following tips to make the best nursing progress notes;
Maintain consistency
The record begins with the ID information of the patient. Each entry should include the following;
- Complete name of the patient
- The time
- The date
Write down timely information
Within 24 hours of supervising your patient, you should write down your notes. This indicates that you have already completed the notes for the next nurse whom shift is next.
Use legible handwriting
The notes should be written neatly and clearly. Since these notes are made for quick reading so you should not writing down lengthy details.
Document all of your communications
Keep in mind that you have to write everything significant concerning the health of the patient. All the conversations that you have with the doctors, family members, and any other medical professional should be included in it.
Avoid using abbreviations
Don’t use abbreviations because they might mean different things to different people. Also, this may lead to miscommunications.
Write as you go
It is the responsibility of the nurse to complete all of their notes as soon as possible. You don’t have to leave your notes until the end of your shift.

How to structure nursing notes?
SBAR method (Situation, Background, Assessment, and Recommendations) is used to structure the nursing notes appropriately.
Situation
Write a sentence to inform the people that what the note is attempting to address. At the start, there is a straightforward summary which informs the reader’s nature of the situation.
Background
In the background, state the origin of the patient’s condition precisely and the treatment was given to the patient in the past. There should be a clear information in this section so that the medical professionals know what next actions they should take for the patient.
Assessment
With the help of a scientific data, you have to provide an opinion in this section. Include the raw data found here. After the assessment, the clinical evaluation should be used to make recommendations. Next, register the findings after the clinical evaluation and then write the relevant clinical results of the patient.
Recommendations
The recommendations or actions that would be taken next depend on the clinical evaluation. Recommendations should be effective and have space for other questions or issues. In order to make clear and compelling content, you should always re-read and edit the nursing notes.
Conclusion:
In conclusion, a nursing note template is an effective tool for nurses to write down their observations about patients. These notes have a patient’s general and basic information. They also give a complete picture of the patient’s health.